IRIS >
IRIS CSV
CSV Template
Form Type,Tax Year,Payer TIN Type,Payer Taxpayer ID Number,Payer Name Type,Payer Business or Entity Name Line 1,Payer Business or Entity Name Line 2,Payer First Name,Payer Middle Name,Payer Last Name (Surname),Payer Suffix,Payer Country,Payer Address Line 1,Payer Address Line 2,Payer City/Town,Payer State/Province/Territory,Payer ZIP/Postal Code,Payer Phone Type,Payer Phone,Payer Email Address,Policyholder TIN Type,Policyholder Taxpayer ID Number,Policyholder Name Type,Policyholder Business or Entity Name Line 1,Policyholder Business or Entity Name Line 2,Policyholder First Name,Policyholder Middle Name,Policyholder Last Name (Surname),Policyholder Suffix,Policyholder Country,Policyholder Address Line 1,Policyholder Address Line 2,Policyholder City/Town,Policyholder State/Province/Territory,Policyholder ZIP/Postal Code,Office Code,Form Account Number,Box 1 - Gross long-term care benefits paid,Box 2 - Accelerated death benefits,Box 3 - Per diem/Reimbursed amount,Insured's TIN Type,Insured's Taxpayer ID Number,First Name,Middle Name,Last Name (Surname),Suffix,Country,Address Line 1,Address Line 2 (optional),City/Town,State/Province/Territory,ZIP/Postal Code,Box 4 - Qualified contract,Box 5 - Chronically ill/Terminally ill,Date Certified
,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,
CSV Columns
Form Type
Tax Year
Payer TIN Type
Payer Taxpayer ID Number
Payer Name Type
Payer Business or Entity Name Line 1
Payer Business or Entity Name Line 2
Payer First Name
Payer Middle Name
Payer Last Name (Surname)
Payer Suffix
Payer Country
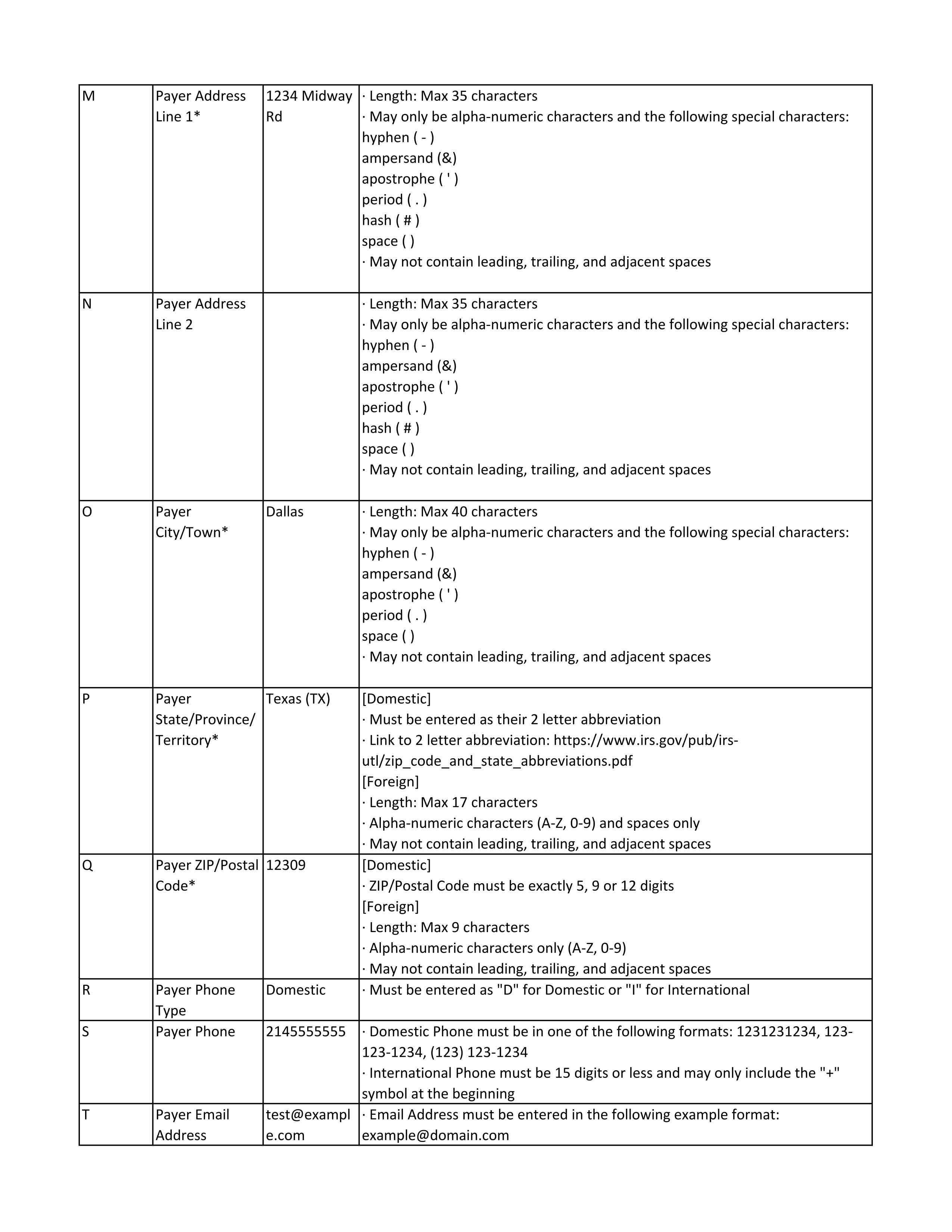
Payer Address Line 1
Payer Address Line 2
Payer City/Town
Payer State/Province/Territory
Payer ZIP/Postal Code
Payer Phone Type
Payer Phone
Payer Email Address
Policyholder TIN Type
Policyholder Taxpayer ID Number
Policyholder Name Type
Policyholder Business or Entity Name Line 1
Policyholder Business or Entity Name Line 2
Policyholder First Name
Policyholder Middle Name
Policyholder Last Name (Surname)
Policyholder Suffix
Policyholder Country
Policyholder Address Line 1
Policyholder Address Line 2
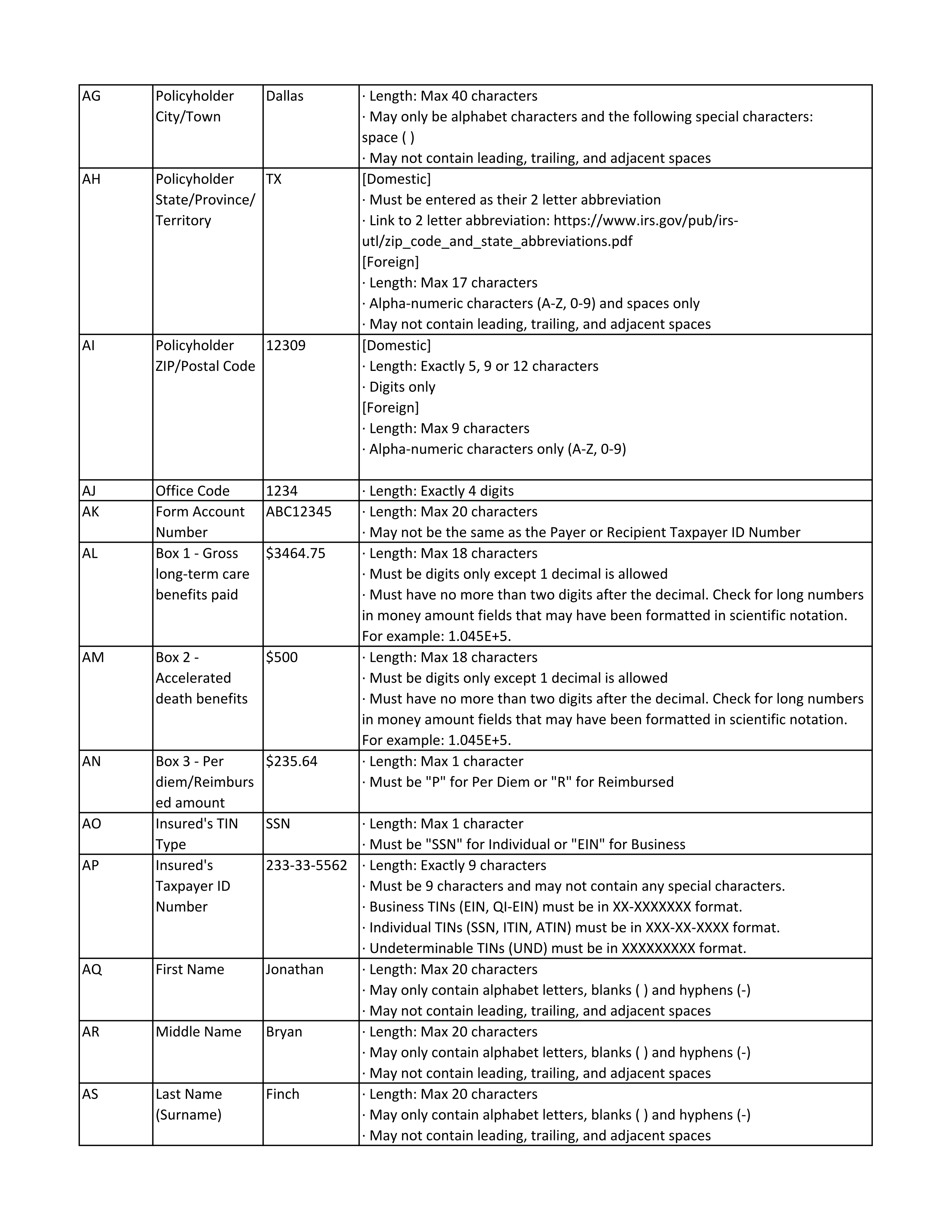
Policyholder City/Town
Policyholder State/Province/Territory
Policyholder ZIP/Postal Code
Office Code
Form Account Number
Box 1 - Gross long-term care benefits paid
Box 2 - Accelerated death benefits
Box 3 - Per diem/Reimbursed amount
Insured's TIN Type
Insured's Taxpayer ID Number
First Name
Middle Name
Last Name (Surname)
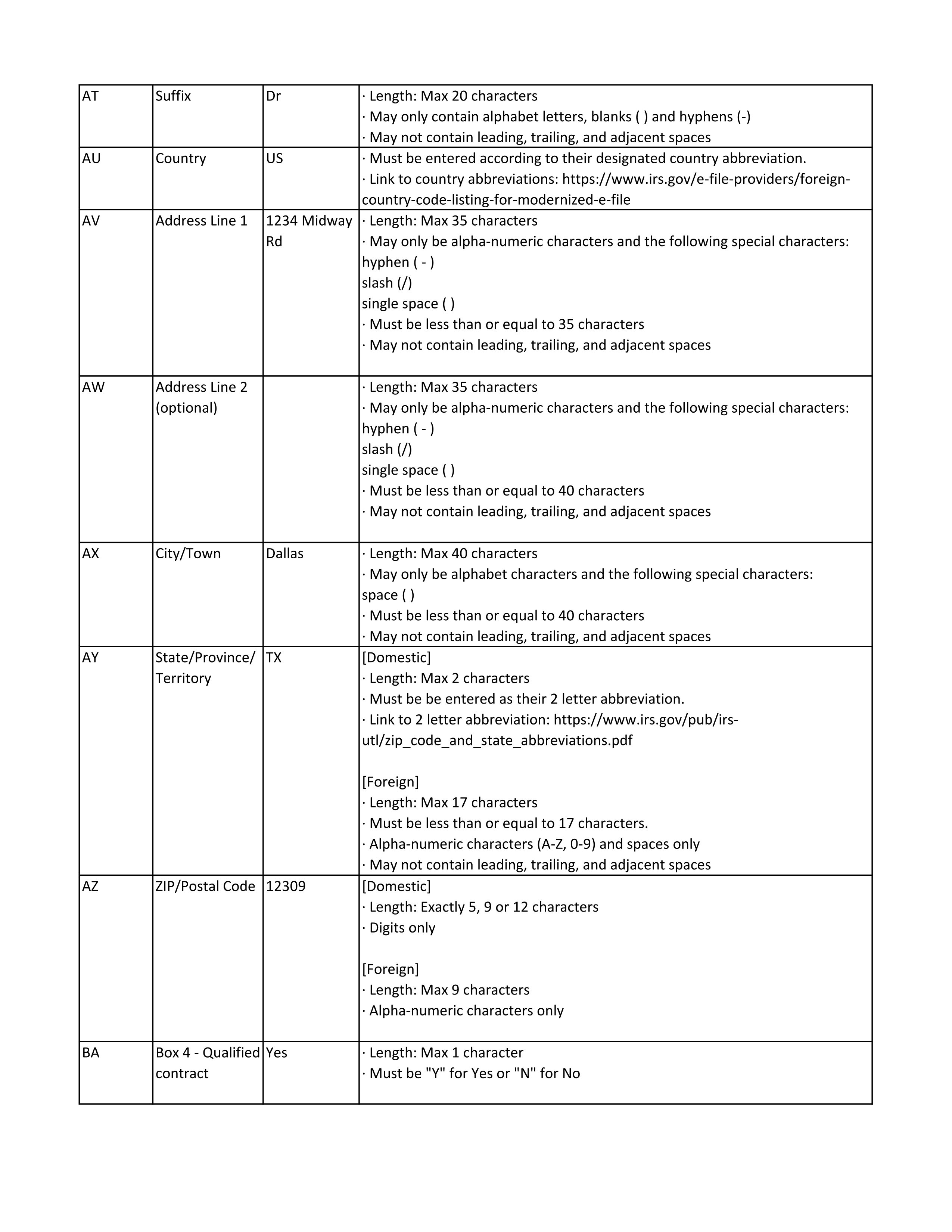
Suffix
Country
Address Line 1
Address Line 2 (optional)
City/Town
State/Province/Territory
ZIP/Postal Code
Box 4 - Qualified contract
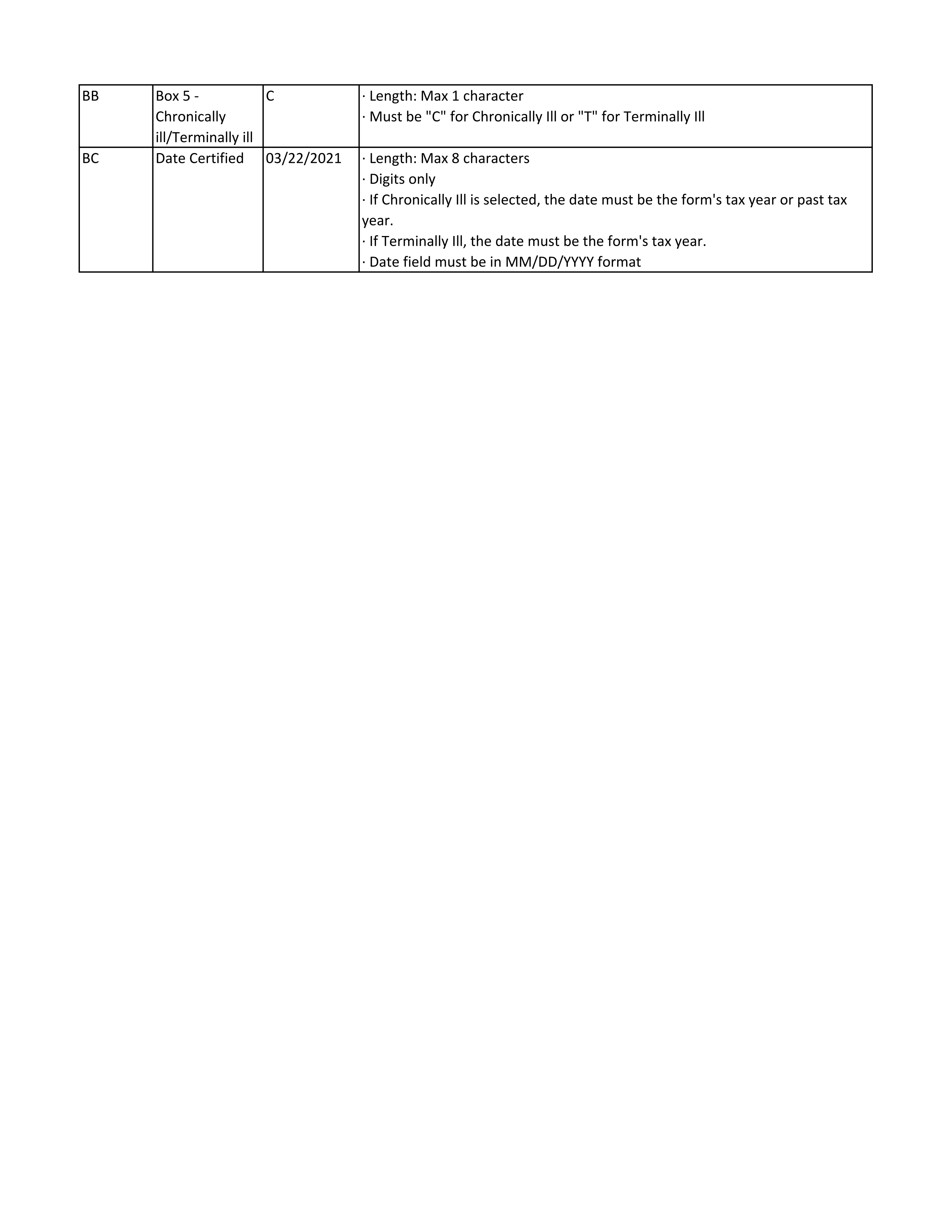
Box 5 - Chronically ill/Terminally ill
Date Certified
CSV Guidelines