1095-A : Health Insurance Marketplace Statement
FDX
FDX / Data Structures / Tax1095A
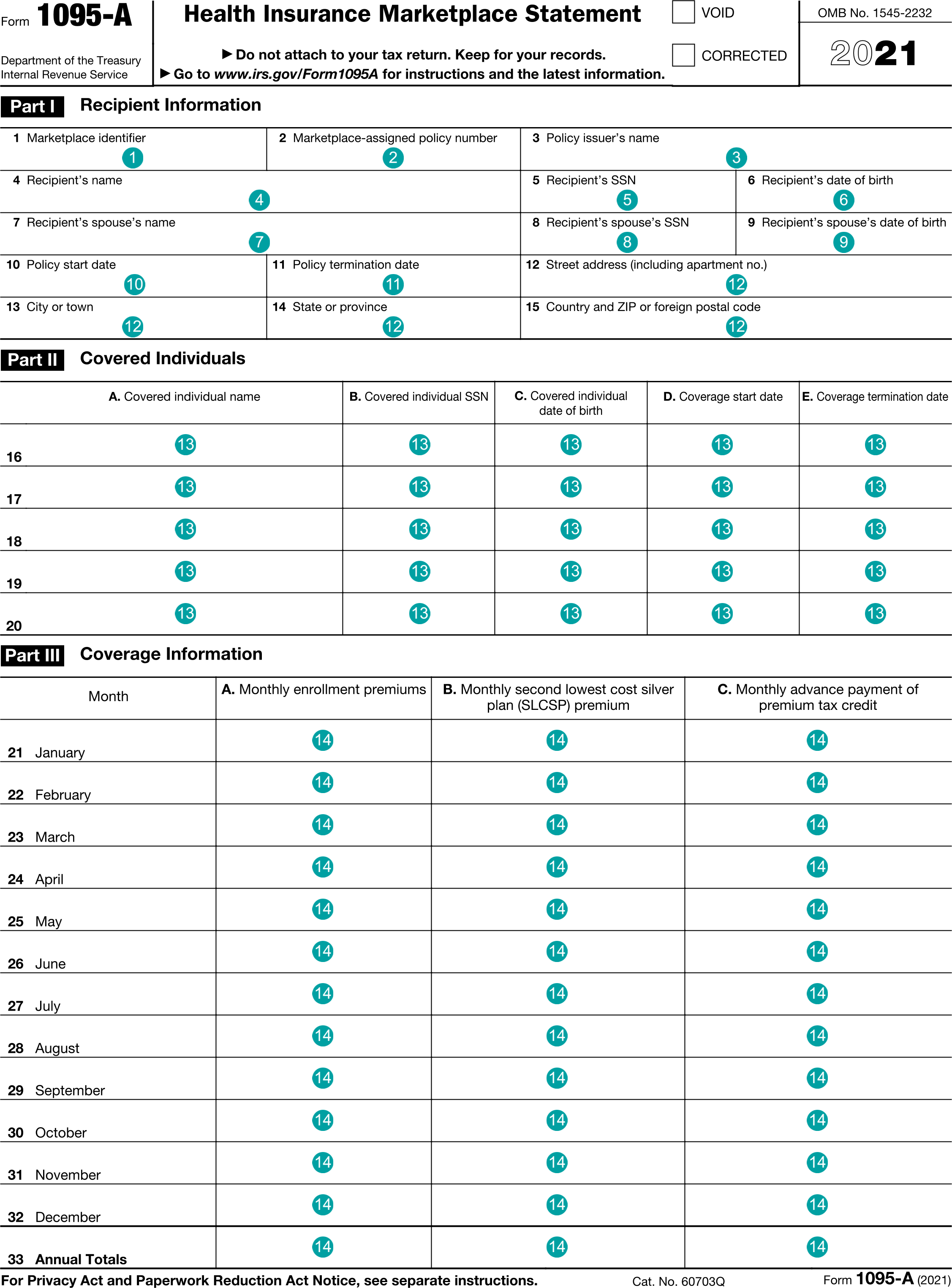
Form 1095-A, Health Insurance Marketplace Statement
Extends and inherits all fields from Tax
Tax1095A Properties
| # | Id | Type | Description |
|---|---|---|---|
| 1 | marketplaceId | string | Box 1, Marketplace identifier |
| 2 | marketplacePolicyNumber | string | Box 2, Marketplace-assigned policy number |
| 3 | policyIssuerName | string | Box 3, Policy issuer's name |
| 4 | recipientName | string | Box 4, Recipient's name |
| 5 | recipientTin | string | Box 5, Recipient's SSN |
| 6 | recipientDateOfBirth | DateString | Box 6, Recipient's date of birth |
| 7 | spouseName | string | Box 7, Recipient's spouse's name |
| 8 | spouseTin | string | Box 8, Recipient's spouse's SSN |
| 9 | spouseDateOfBirth | DateString | Box 9, Recipient's spouse's date of birth |
| 10 | policyStartDate | DateString | Box 10, Policy start date |
| 11 | policyTerminationDate | DateString | Box 11, Policy termination date |
| 12 | recipientAddress | Address | Boxes 12-15, Recipient address |
| 13 | coveredIndividuals | Array of HealthInsuranceMarketplaceCoveredIndividual | Boxes 16+, Covered Individuals |
| 14 | coverages | Array of HealthInsuranceCoverage | Boxes 21-33, Coverage Information |
Tax1095A Usage:
- TaxData tax1095A
OFX
OFX / Types / Tax1095A_V100
| # | Tag | Type |
|---|---|---|
| 1 | SRVRTID | ServerIdType |
| 2 | TAXYEAR | YearType |
| 3 | VOID | BooleanType |
| 4 | CORRECTED | BooleanType |
| 5 | MARKETPLACEIDENTIFIER | GenericNameType |
| 6 | MARKETASSIGNEDPOLICYNUM | GenericNameType |
| 7 | POLICYISSUERNAME | GenericNameType |
| 8 | RECIPIENTINFO | RecipientInfo |
| 9 | POLICYSTARTDATE | DateTimeType |
| 10 | POLICYTERMINATIONDATE | DateTimeType |
| 11 | COVERAGEHOUSEHOLD | CoverageHouseholdType |
| 12 | HOUSEHOLDINFO | HouseholdInformationType |
| 13 | TOTALPLANPREMIUMAMT | AmountType |
| 14 | TOTALPREMIUMSLCSPAMT | AmountType |
| 15 | TOTALADVANCEPTCAMT | AmountType |
Usages:
- Tax1095Response TAX1095A_V100
FIRE
This form is not reported in the IRS FIRE system.
TXF
The TXF standard does not support this form.